When a baby’s mouth is forming in the womb, the tongue, lip and cheeks are connected to the gums and jawbone with tissue called a frenulum. Everyone has a frenulum under their tongue, under their upper lip, and on parts of their cheeks. It is often normal and without associated medical problems.
When a frenulum impacts function, it is called a tongue tie (also known as ankyloglossia) and other oral ties (such as to the lip or cheeks) can be present. A frenulum is considered tethered or “tied” if a tight or restricted frenulum causes restriction in function for breastfeeding, eating, drinking or speaking. It is considered a normal frenulum if there is no restriction in function.
Tongue-tie or Ankyloglossia
Tongue-tie or Ankyloglossia, happens when the lingual (tongue) frenulum tissue that attaches the tongue to the lower jaw is too short or thick, limiting the full movement of the tongue and this impacts breastfeeding, eating, speech and oral hygiene (but not necessarily formation of dental caries). Current studies are also looking at the impact of tongue tie on facial growth and oral/dental development, as well as airway development and mouth breathing.
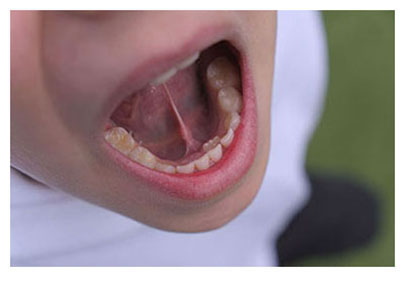
Photo above-right: tethered oral tissues may be associated with dental crowding and underdevelopment of the jaw
How do I know if my tongue frenum is restricted?
- Open your mouth as wide as you can, then lift your tongue up towards your top jaw and take note of how far the tongue can lift.
- Gently place your finger on the floor of your mouth (the area between your lower jawbone and the undersurface of the tongue) and try to lift your tongue again.
If the elevation is limited, you may want to consult a professional trained in tongue tie diagnosis and treatment to help you assess options for care, especially if you have trouble with things like chewing or swallowing food or drink, saying certain sounds, breathing issues or other dental concerns like crowding of teeth or baby teeth that do not fall out on their own.
Lip tie (or Labial Frenulum)
Lip tie (or Labial Frenulum) occurs when the lip (labial) tissue that connects the upper lip to the gums on the upper jawbone is too tight, thick, or short, which can impact oral development, and spacing of erupting teeth. Current studies are also looking at the impact of a lip tie on speech and breastfeeding difficulties.
Cheek tie (Buccal tie)
Cheek tie (Buccal tie) is when there is restrictive frenulum tissue from soft tissue of cheeks to the bony part of the upper or lower jaw. There are no current measurement systems available to categorize cheek ties. Research is ongoing right now to better understand the impact of these ties and whether they are necessary to treat.